Article Text

Abstract
Objective The cardiovascular manifestations of Fabry disease are common and represent the leading cause of death. Disease-specific therapy, including enzyme replacement therapy (ERT) and chaperone therapy (migalastat), is recommended for patients exhibiting cardiovascular involvement, but its efficacy for modulating cardiovascular disease expression and optimal timing of initiation remains to be fully established. We therefore aimed to systematically review and evaluate the effectiveness of disease-specific therapy compared with placebo, and to no intervention, for the cardiovascular manifestations of Fabry disease.
Methods Eight databases were searched from inception using a combination of relevant medical subject headings and keywords. Randomised, non-randomised studies with a comparator group and non-randomised studies without a comparator group were included. Studies were screened for eligibility and assessed for bias by two independent authors. The primary outcome comprised clinical cardiovascular events. Secondary outcomes included myocardial histology and measurements of cardiovascular structure, function and tissue characteristics.
Results 72 studies were included, comprising 7 randomised studies of intervention, 16 non-randomised studies of intervention with a comparator group and 49 non-randomised studies of intervention without a comparator group. Randomised studies were not at serious risk of bias, but the others were at serious risk. Studies were highly heterogeneous in their design, outcome measurements and findings, which made assessment of disease-specific therapy effectiveness difficult.
Conclusion It remains unclear whether disease-specific therapy sufficiently impacts the cardiovascular manifestations of Fabry disease. Further work, ideally in larger cohorts, with more standardised clinical and phenotypic outcomes, the latter measured using contemporary techniques, are required to fully elucidate the cardiovascular impact of disease-specific therapy.
PROSPERO registration number CRD42022295989.
- Cardiomyopathies
- Cardiomyopathy, Hypertrophic
- Genetic Diseases, Inborn
- Metabolic Diseases
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Disease-specific therapy, including enzyme replacement therapy and chaperone therapy (migalastat), is recommended for patients exhibiting cardiovascular involvement, but its efficacy for modulating cardiovascular disease expression, optimal timing of initiation and cost-effectiveness remain to be fully established.
WHAT THIS STUDY ADDS
Studies that evaluate the effectiveness of disease-specific therapy, compared with placebo, and to no intervention, for the cardiovascular manifestations of Fabry disease are highly heterogeneous in their design, outcome measurements and findings, which makes assessment of disease-specific therapy effectiveness difficult.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
It remains unclear whether disease-specific therapy sufficiently impacts the cardiovascular manifestations of Fabry disease. Further work, ideally in larger cohorts, with more standardised clinical and phenotypic outcomes, the latter measured using contemporary techniques, are required to fully elucidate the cardiovascular impact of disease-specific therapy.
Introduction
Fabry disease is a rare X-linked lysosomal storage disorder characterised by deficiency of alpha-galactosidase and the accumulation of its substrate, globotriaosylceramide (Gb3).1 The cardiovascular manifestations, which include myocardial hypertrophy, fibrosis and ischaemia, and arrhythmia, are common, affecting more than 50% of males and females, and represent the leading cause of death.2 3
Disease-specific therapy, including enzyme replacement therapy (ERT) or chaperone therapy (migalastat), is recommended for patients exhibiting cardiovascular involvement, but its efficacy, optimal timing of initiation and cost-effectiveness are yet to be fully elucidated.
Previous systematic reviews are limited by the exclusion of chaperone therapy, which has been part of routine clinical practice for over 5 years, and the exclusion of non-randomised studies, which account for much of the published data.4 5 Furthermore, by evaluating effectiveness in Fabry disease in general, evaluation of the cardiovascular impact of disease specific therapy has been relatively limited.
Objective
This study aimed to systematically review and evaluate the effectiveness of disease-specific therapy, compared with placebo, and to no intervention, for the cardiovascular manifestations of Fabry disease.
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.6 The search strategy was constructed by a multidisciplinary team (cardiologists, metabolic physicians, specialist librarians). Eligible studies were grouped into randomised studies of intervention, non-randomised studies of intervention with a comparator group and non-randomised studies of intervention without a comparator group (uncontrolled before and after studies). The protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO); CRD42022295989. Further information is available in the online supplemental materials.
Supplemental material
Results
Study selection
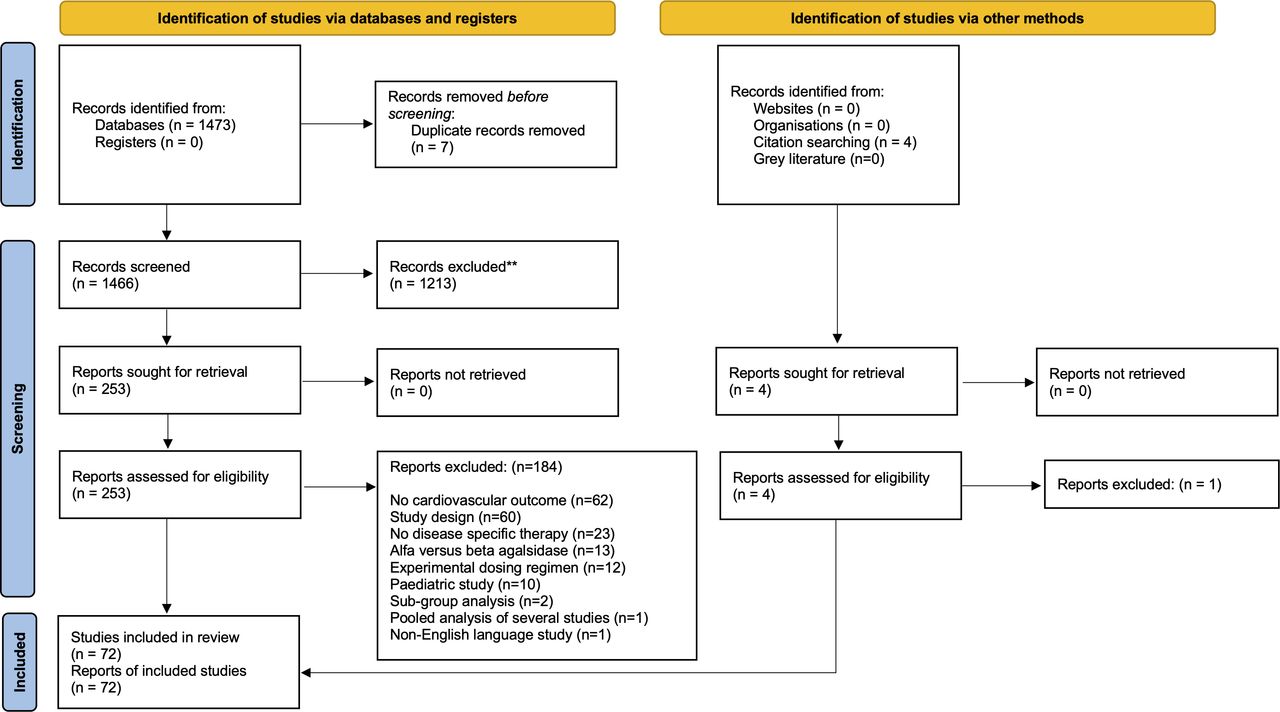
The study selection process is reported in figure 1. The review included 72 studies: 7 randomised studies of intervention, 16 non-randomised studies of intervention with a comparator group and 49 non-randomised studies of intervention without a comparator group (online supplemental tables 1–3, figure 1). Study characteristics are detailed in the online supplemental materials.

PRISMA diagram. PRISMA flow diagram including searches of databases, registers and other sources. PRISMA, Preferred Reporting Items for Systematic Review and Meta-Analysis.
Assessment of risk of bias
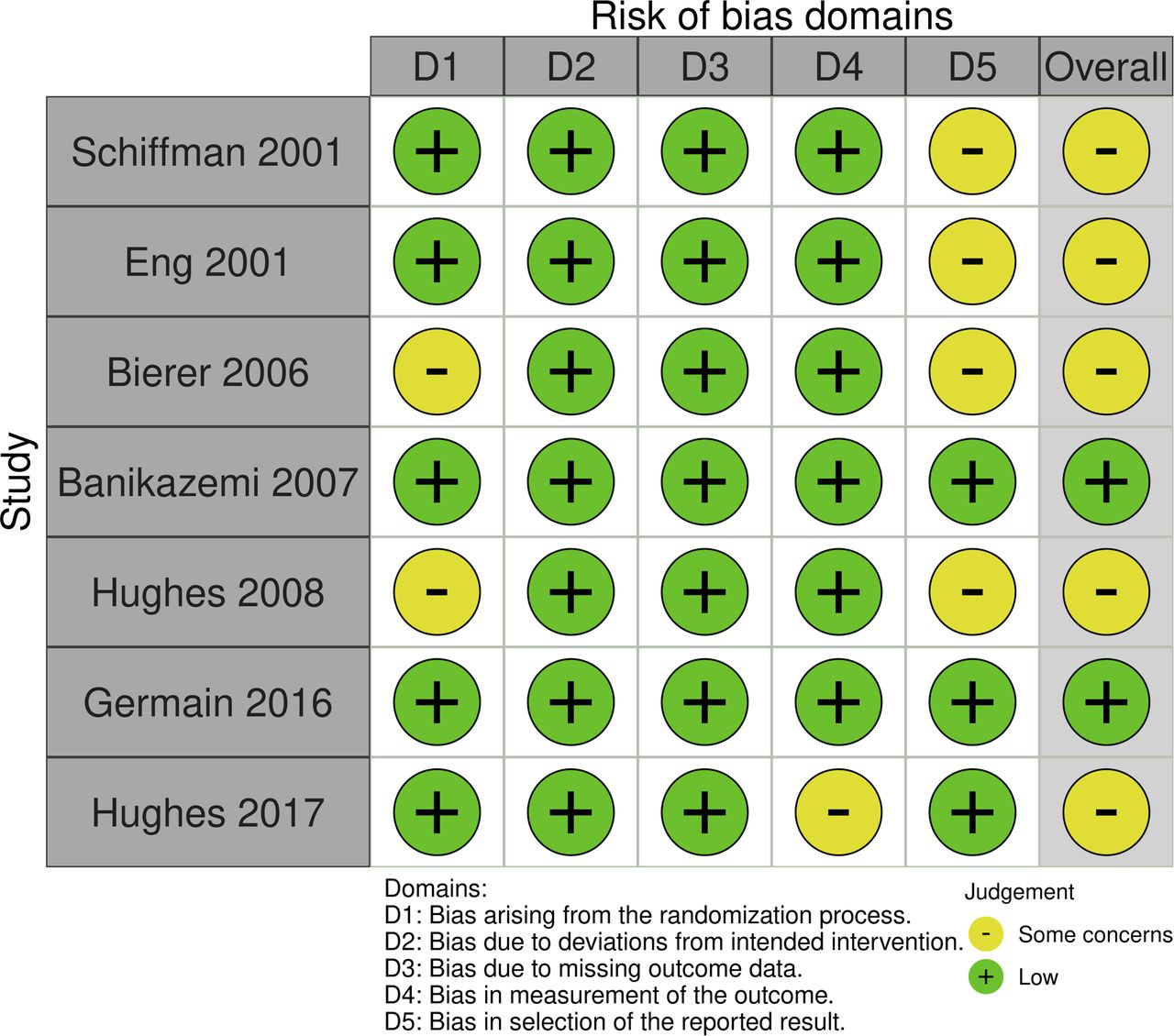
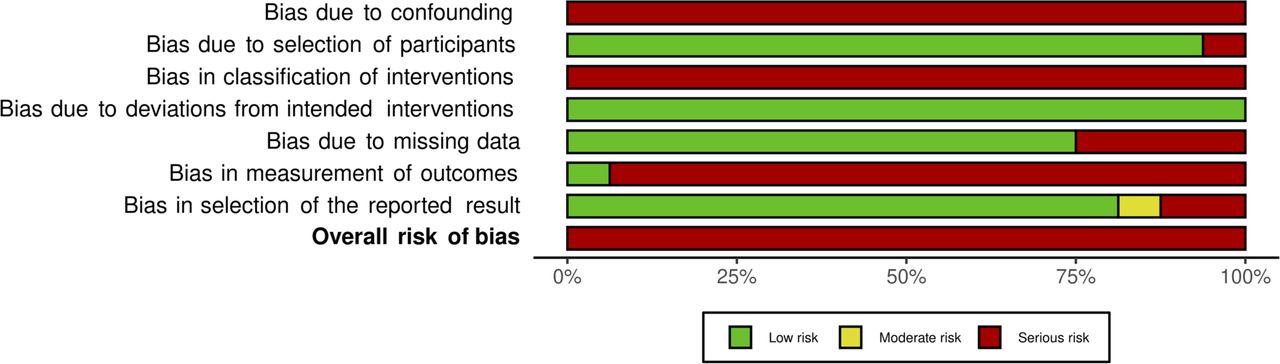
The bias assessment of the randomised studies of intervention (figures 2 and 3) showed two studies were at ‘low risk’ of bias and five studies had ‘some concerns’ due to a risk of bias in the randomisation process (domain 1) or a risk of bias in selection of the reported result (domain 5). The bias assessment of the non-randomised studies of intervention with a comparator group (figures 4 and 5) demonstrated that all studies were at serious risk of bias. All non-randomised studies of intervention without a comparator group were found to be at serious risk of bias because, for example, it is not possible to determine whether study findings are secondary to the intervention.7 Additional information is available in the online supplemental materials.

Traffic light plot of the risk of bias assessment, evaluated using the RoB2 and robvis tools. Traffic light plot displaying risk of bias in multiple domains generated using the revised tool for a revised Cochrane risk of bias tool for randomised trials (RoB2) and the Risk of bias VISualisation tool (robvis).

Summary plot of the risk of bias assessment, evaluated using the RoB2 and robvis tools. Summary plot displaying risk of bias in multiple domains generated using the revised tool for a revised Cochrane risk of bias tool for randomised trials (RoB2) and the Risk of bias VISualisation tool (robvis).

Traffic light plot of the risk of bias assessment, evaluated using the ROBINS-I tool. Traffic light plot displaying risk of bias in multiple domains generated using the tool for assessing Risk Of Bias In Non-randomised Studies of Interventions (ROBINS-I) and the Risk of bias VISualisation tool.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary plot of the risk of bias assessment, evaluated using the risk of bias tool for randomised trials tool, displaying risk of bias in multiple domains generated using the tool for assessing Risk Of Bias In Non-randomised Studies of Interventions and the Risk of bias VISualisation tool.
Results of synthesis
In the presence of substantial heterogeneity in study design and study outcome, as here, statistical pooling and meta-analysis are not recommended. A narrative synthesis was therefore conducted, which first considers ERT and subsequently chaperone therapy.7
Enzyme replacement therapy
Clinical cardiovascular outcomes
A double-blind placebo randomised control trial (RCT) of agalsidase beta demonstrated no change in time to a composite clinical outcome (renal, cardiac, cerebrovascular events or death) during 18.4±8.8 months follow-up in 82 patients (HR 0.47 (0.21–1.03); p=0.06), and no change in time to a composite clinical cardiovascular outcome (HR 0.42 (0.058–2.7); p=0.42), although the number of cardiovascular events were small (three in the interventional arm and four in the placebo arm). However, a secondary analysis of 74 protocol-adherent patients did demonstrate an increase in time to first composite clinical outcome in the agalsidase beta group (HR 0.39 (0.16–0.93); p=0.034).8
A 5-year, non-randomised study observed no change in time to first complication in 58 patients in an ERT cohort compared with 42 patients in a natural history cohort (p=0.69), although the risk of developing a first complication declined with longer treatment duration (OR 0.81 (0.68–0.96) per year; p=0.015). Cardiovascular events were not specifically reported.9
Weidemann et al10 found no difference in clinical outcome (stroke, end-stage renal disease, dialysis and death) in patients treated with ERT compared with a natural history cohort (untreated adult patients matched by year of birth, gender, previous transient ischaemic attack and chronic kidney disease stage) (HR 1.48; 95% CI 0.72 to 3.06; p=0.284) although cardiovascular events were not reported. Beck et al,11 who compared 79 patients derived from a registry with 31 patients from a double-blind placebo RCT, found a 16% risk of a composite morbidity outcome after 24 months in patients receiving ERT versus 45% in the placebo group. Age of first event and death was also higher in the ERT group. Cardiovascular events were not reported.11 Many single-arm studies report the frequency of clinical outcomes but without a comparator group, precluding evaluation of the impact of ERT.
LV mass and wall thickness
Some studies have reported a significant reduction in left ventricular (LV) mass with ERT. For example, a 6-month double-blind placebo RCT of agalsidase alfa in 15 patients with left ventricular hypertrophy (LVH) at baseline demonstrated a reduction in left ventricular mass index (LVMI), measured using cardiovascular magnetic resonance (CMR) (−6.4 g/m2 vs +12 g/m2; p=0.02), although there was no further reduction in LVM in a 24-month open-label extension (n=10).12 Moreover, in a study including 181 participants with 5-year echocardiographic data taken from a larger cohort of 1428 patients, Mehta et al13 demonstrated a significant reduction in LVMI during the first 3 years of agalsidase alfa (−6.3 g/m2.7, p=0.0085). Subgroup analysis revealed this reduction was confined to patients with LVH. Similarly, Kampmann et al14 observed a significant reduction in LVMI in males with LVH after 10.8 years (range 9.6–12.5) of treatment with agalsidase alfa (−13.55 g/m2.7 (−23.05 to −4.06), n=15; p=0.0061). There was no change in males without LVH and no change in females.
Other studies report significant slowing of LV mass progression with ERT. For example, a non-randomised study comparing 164 ERT-treated patients with a published dataset of 78 untreated patients demonstrated a reduced rate of LVMI progression during 5.2-year follow-up (treated males 0.33±0.10 g/m2/year vs untreated males 4.07±1.03 g/m2/year; treated females 0.48±0.09 g/m2/year vs untreated females 2.31±0.81 g/m2/year).11 Similarly, after adjusting for baseline LVMI, Hongo et al15 demonstrated a reduced rate of LVMI progression in 42 patients treated with ERT compared with the same untreated dataset (treated males 1.59±1.23 g/ht2.7/year vs untreated males 4.07±1.03 g/ht2.7/year; treated females 1.00±1.25 g/ht2.7/year vs untreated females 2.31±0.81 g/ht2.7/year; p<0.01).15 Nordin et al16 found LVMI did not change significantly over 12 months of ERT in patients either initiating ERT (93±42 g/m2 to 92±40 g/m2; p=0.186) or established on ERT (124±45 g/m2 to 125±45 g/m2; p=0.070), whereas LVMI did increase in untreated patients (65±15 g/m2 to 67±16 g/m2; p=0.005). Furthermore, a study of 311 ERT-treated patients demonstrated an association between ERT duration and decrease in LVMI (p=0.01).17
In other studies, a stabilisation of LV mass progression with ERT is suggested, but without a comparator group to benchmark. For example, Germain et al18 observed LV wall thickness to be relatively unchanged, and within normal limits, over 10 years of agalsidase beta therapy (posterior wall thickness 10.6±2.3 mm to 11.7±3.0 mm; interventricular septum 10.7±2.3 mm to 11.5±3.1 mm; n=50).
In comparison, other studies have not identified a significant impact of ERT on LV mass. For example, Madsen et al19 demonstrated no significant change in LVMI or wall thickness in 47 patients treated with ERT for 8 years compared with 19 untreated patients (ERT: 102 g/m2 (range 54–231 g/m2) to 97g/m2 (47–306 g/m2), p=0.31; no ERT: 89 g/m2 (50–271 g/m2) to 104 g/m2 (55–328 g/m2), p=0.57). Likewise, Krämer et al,20 who compared 57 ERT-treated and 16 untreated patients, found no significant change in LVMI or wall thickness during 4.8±2.4 year follow-up (ERT: 92±33 g/m2 to 90±30 g/m2; p>0.05, no ERT: 59±11 g/m2 to 61±14 g/m2; p>0.05). Vijapurapu et al21 demonstrated similar LVM progression over 37 months (20–60) in ERT-treated (n=50) compared with untreated (n=45) patients (males: ERT+2.5%/year vs untreated+1.9%/year; females: ERT+0.9%/year vs untreated+1.1%/year), and a post-marketing study by Sasa et al that included 493 patients did not demonstrate any significant change in LVMI at 3 or 5 years (n=72, n=20, respectively).22 23 In a subsequent analysis of the cohort described above (Mehta et al), this time including 250 patients selected from the larger cohort, there was no change in LVMI in males over 4 years (54.7±24.0 g/m2.7 to 52.2±19.2 g/m2.7, n=45; p=0.247).22 There did remain a significant reduction in LVMI in females (48.2±17.0 g/m2.7 to 43.7±14.3 g/m2.7, n=24; p=0.031). Furthermore, a registry including 115 ERT-treated and 48 untreated males found no difference in annual change in LVM, except in a subgroup in whom ERT was initiated between age 18 and 29 years.24
Cardiac histology, myocardial T1 relaxation time, late gadolinium enhancement, LV function, myocardial T2 relaxation time, myocardial extracellular volume, myocardial perfusion, myocardial energetics, aortic size, cardiac electrophysiology, exercise capacity and right ventricular structure and function
Please see online supplemental materials.
Chaperone therapy
A 6-month double-blind placebo RCT demonstrated a reduction in LVMI with migalastat (93.3±30 g/m2 to 92.9±29 g/m2; n=28) compared with an increase with placebo (101.7±37 g/m2 to 108±51 g/m2; n=22), although the difference was not statistically significant.25 A subsequent open-label extension of up to 24 months, in which all patients received migalastat, demonstrated a significant reduction in LVMI from baseline (−7.7 g/m2 (−15.4 to −0.01 g/m2)).25
An 18-month RCT of migalastat (n=36) versus ERT (n=21) demonstrated a significant reduction in LVMI from baseline in patients receiving migalastat (−6.6 g/m2 (−11.0 to −2.2 g/m2)) but not in patients receiving ERT (−2.0 g/m2 (−11.0 to 7.0 g/m2)). There were no changes in LV function. Clinical cardiac events were infrequent (two in migalastat group; three in ERT group).26 During a 12-month open-label extension in which all patients received migalastat, there was a further reduction in LVMI in patients with LVH originally randomised to migalastat (n=11; −11.3 g/m2 (−16.6 to −3.3 g/m2)).27
Two non-randomised studies without comparators demonstrated reductions in LVMI 14 and 24 months, respectively, after commencing migalastat (Müntze et al28: 137 g/m2 (86–159 g/m2) to 130 g/m2 (82–169 g/m2), n=14; p=0.012; Lenders et al29: 109.5±47.3 g/m2 to 102.0±40.0 g/m2, n=54; p=0.0118). There was no change in high-sensitivity troponin T or N-terminal pro B-type natriuretic peptide.28
Discussion
This systematic review evaluated the effectiveness of disease-specific therapy compared with placebo, and to no intervention, for the cardiovascular manifestations of Fabry disease.
The included studies were heterogeneous in design, size, comparator, risk of bias and outcome. The ERT RCTs (n=5) and chaperone therapy RCTs (n=2) were small, and in the case of ERT, under-represented females (ERT: 183 males and 13 females, migalastat: 49 males and 75 females), but were not at serious risk of bias. The 16 non-randomised studies of ERT with a comparator group were all at serious risk of bias. Comparator groups included patients not requiring disease-specific therapy, who presumably had milder phenotypes although treatment criteria varied considerably, previously published datasets, ‘natural history’ cohorts and interrupted time-series analyses. There were no non-randomised studies of chaperone therapy with a comparator group. The remaining 49 studies (ERT 45; chaperone therapy 4) were non-randomised studies of intervention without a comparator group, and all were at serious risk of bias.
Studies were predominantly small and single-centre, although the non-randomised ERT studies included large international registries. Inclusion criteria (eg, all-comers vs exclusively males,24 exclusively females,30 or patients with pre-existing cardiac or renal disease),8 12 duration (20 weeks to 10 years), and analysis methodology (eg, within-group comparisons, between-group comparisons, stratification by variables such as age,24 sex or LVH,13 open-label extensions) were highly variable, and many reported salient levels of missing data.
Outcome measurements were particularly heterogeneous. Clinical cardiovascular events were seldom reported and were infrequent when they were reported, precluding meaningful analysis. LV mass assessments comprised the most common endpoints (65 studies), although these were also inconsistent, including LV mass, LV mass indexed to body surface area, LV mass indexed to height12 13 19 and surrogates of LV mass including septal, posterior wall and segmental thickness (online supplemental reference 1).30 The level of heterogeneity made effectiveness of disease-specific therapy difficult to assess.
In a series of publications with increasing follow-up duration relating to a 20-week placebo RCT, ERT was consistently associated with a reduction in cardiac endothelial Gb3 (online supplemental references 2 and 3), although this is the only study to evaluate the impact of disease-specific therapy on cardiac endothelial Gb3. ERT was not associated with a reduction in myocardial Gb3 (online supplemental reference 2).12
Data regarding the impact of disease-specific therapy on cardiac phenotype are inconsistent. A number of studies found ERT and chaperone therapy to reduce or slow the progression of measurements of LV mass, predominantly in patients with LVH at baseline. However, other studies did not identify a significant impact of disease-specific therapy on measurements of LV mass. The reasons for the variable results are unclear, but may include differences in participant characteristics, duration of therapy and differential treatment response. In most studies, assessment of LV mass was made using echocardiography. The limited accuracy and high variability of echocardiography-derived LV mass, particularly in the context of variable ventricular geometry, such as is evident in Fabry disease, is well described (online supplemental reference 4), and measurement of LV wall thickness, even when performed using CMR images, is highly variable (online supplemental reference 5). Together with the small sample sizes and often short duration, many studies may not have been sensitive to relatively small changes in LV mass, especially considering the slowly progressive nature of Fabry disease.
In other conditions, tissue characterisation with CMR has identified myocardial injury and disease expression in advance of changes in ‘macro’ structure and function, such as LV mass or ejection fraction (online supplemental reference 6). In line with this, myocardial T1 relaxation time is a putative non-invasive biomarker of Gb3 accumulation. The available studies suggested that ERT may possibly be associated with an improvement in T1 relaxation time, however, data were very limited and somewhat inconsistent.16 21 Data regarding the impact of disease-specific therapy on LGE, a measure of focal myocardial fibrosis, were also very limited (online supplemental references 7 and 8).16
Previous systematic reviews focus exclusively on ERT and have been variable in their conclusions. A Cochrane review of RCTs concluded that the long-term influence of ERT on risk of morbidity and mortality remains to be established.5 Two recent systematic literature reviews incorporating observational data concluded that in males: ‘data published in adult male patients with Fabry disease demonstrates that the effect of ERT on plasma Gb3 levels, eGFR, and cardiac outcomes is strongest and substantiated by a wide range of publications, showing consistent, dose-dependent reductions in Gb3 accumulation, a reduced decline in eGFR, and improvements in cardiac outcomes’. Whereas in females: ‘ERT in adult female patients with Fabry disease has a beneficial effect on Gb3 levels and cardiac outcomes’ (online supplemental references 9 and 10). A meta-analysis concluded that ERT did have a beneficial effect on the course of LV mass when compared with untreated groups (online supplemental reference 11). Specifically, in males with LVH at baseline LV mass remained stable, whereas in males without LVH at baseline the rate of LVH progression was lower than in untreated patients. In females with LVH at baseline LV mass decreased, and in females without LVH at baseline, LV mass remained stable compared with an increase in untreated patients. Importantly however, this meta-analysis included data from only 6 of 64 studies that report LV mass (online supplemental reference 11).
Given the marked heterogeneity of study design and outcome measurements, the relatively small sample size of most studies and low reported clinical event rates, the risk of study bias and the rare and slowly progressive nature of the condition, it remains unclear whether disease-specific therapy sufficiently impacts the cardiovascular manifestations of Fabry disease, particularly in the context of the not inconsiderable associated cost.
In future, large, statistically powered, multi-centre, prospective studies assessing the efficacy of therapy using standardised outcomes are required. The impact of disease-specific therapy on pre-defined ‘hard’ clinical cardiovascular outcomes, such as sudden cardiovascular death or malignant ventricular arrhythmia must be prioritised and additional secondary phenotypic outcomes derived from contemporary imaging, circulating biomarker and heart rhythm techniques should be measured using contemporary techniques. Moreover, if these secondary phenotypic outcomes are to be meaningful, their prognostic significance must be understood. In particular, the prognostic significance of a change in LVMI and native myocardial T1 relaxation time over time requires further elucidation (online supplemental reference 12). This future work is likely to require international collaboration, expert consensus, patient and patient-group involvement and impartial funding.
A limitation of the current study is that a meta-analysis was not performed; however, the heterogeneity of published studies precluded statistical pooling and meta-analysis. Agalsidase alfa and beta were not considered separately in keeping with most studies. Measurements such as LVMI are subject to variability based on methodological approach (inclusion or exclusion of papillary muscles). Patients receiving disease-specific therapy are generally more severely affected than those who are untreated. Direct or indirect industry involvement is common in Fabry disease studies, reflecting the nature of rare disease research. Study funders are listed in the tables summarising study characteristics (online supplemental tables 1–3). A formal Tool for Addressing Conflicts of Interest in Trials (TACIT) is being developed under the auspices of the Cochrane Bias Methods Group.
Conclusion
This systematic review evaluated the effectiveness of disease-specific therapy compared with placebo, and to no intervention, for the cardiovascular manifestations of Fabry disease. The heterogeneity of the evidence made it difficult to assess the effectiveness of disease-specific therapy, and it remains unclear whether it sufficiently impacts the cardiovascular manifestations. Further work, ideally in larger cohorts, with more standardised clinical and phenotypic outcomes, the latter measured using contemporary imaging, circulating biomarker and heart rhythm techniques, are required to fully elucidate the impact of disease-specific therapy on the cardiovascular manifestations of Fabry disease.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors participated in study design and conduct; data acquisition, analysis, and interpretation; drafting and revising the manuscript; and approved the final version before submission. The initial responsibility at each stage, prior to approval from all co-authors, can be attributed to: CAM, AJ, MS, AR and PW for the conception and design of the study; CO and NB for design of the search strategy, study selection, data extraction and assessment of risk of bias; CO, NB and CAM for drafting the manuscript; and all authors critically reviewed and approved the final manuscript. CAM is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS or the UK Department of Health and Social Care.
Competing interests CAM, Advanced Fellowship, NIHR301338 is funded by the National Institute for Health Research (NIHR). This work was also supported in part by a British Heart Foundation Accelerator Award to the University of Manchester (AA/18/4/34221). CAM has served on advisory boards for Novartis, Boehringer Ingelheim and Lilly Alliance and AstraZeneca, serves as an advisor for HAYA Therapeutics and PureTech Health, and has received research support from Amicus Therapeutics, Guerbet Laboratories Limited, Roche and Univar Solutions B.V. MS, AJ and CO have research support from Amicus Therapeutics. All other authors have reported that they have no relationships relevant to the contents of this paper.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.