Article Text

Abstract
Background The impact of early-stage chronic kidney disease (CKD) on cardiovascular outcomes, particularly when albuminuria is present, remains unclear. This study examined the associations between early CKD (stages 1 and 2) with and without albuminuria and the incidence of major adverse cardiovascular events (MACEs), heart failure (HF) and all-cause mortality.
Methods A cohort of 456 015 participants from the UK Biobank was categorised by CKD stage using serum creatinine to calculate estimated glomerular filtration rate (eGFR) and urinary albumin-creatinine ratio (≥3 mg/mmol) to define albuminuria. Multivariable Cox proportional hazard models were applied to evaluate the associations between CKD stages and cardiovascular outcomes. Additionally, left ventricular mass (LVM), an intermediate cardiovascular risk marker, was assessed in a subset of participants using cardiovascular MRI.
Results Compared with normal kidney function, the risk of adverse outcomes increased progressively with advancing CKD stages, except for stage 2 CKD without albuminuria. Stage 2 CKD with albuminuria was associated with higher risks of MACE (HR 1.32, 95% CI 1.25 to 1.38), HF (HR 1.79, 95% CI 1.67 to 1.92) and all-cause mortality (HR 1.51, 95% CI 1.44 to 1.58), comparable to stage 3A CKD without albuminuria. The presence of albuminuria significantly interacted with the relationships between CKD stages and outcomes. No significant differences in indexed LVM were observed between early-stage CKD with albuminuria and normal renal function.
Conclusions In early-stage CKD, albuminuria is independently associated with increased risks of MACE, HF and mortality. These findings support the use of albuminuria over eGFR decline alone for cardiovascular risk stratification in early CKD.
- Risk Factors
- Biomarkers
- Heart Failure
- Cardiovascular Diseases
- Cohort Studies
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data underlying this article were provided by the UK Biobank under access application 2964. UK Biobank will make the data available to bona fide researchers for all types of health-related research that is in the public interest, without preferential or exclusive access for any persons. All researchers will be subject to the same application process and approval criteria as specified by UK Biobank. For more details on the access procedure, see the UK Biobank website (http://www.ukbiobank.ac.uk/register-apply/).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Advanced chronic kidney disease (CKD) is a recognised risk factor for cardiovascular disease (CVD), with albuminuria playing a critical role in prognostication.
However, the cardiovascular impact of early-stage CKD, especially when accompanied by albuminuria, is less well understood.
WHAT THIS STUDY ADDS
This study highlights that albuminuria in early CKD stages (1 and 2) is significantly associated with higher risks of major adverse cardiovascular events, heart failure and all-cause mortality, independent of estimated glomerular filtration rate decline.
Participants with stage 2 CKD and albuminuria exhibited similar cardiovascular risk profiles to those with more advanced CKD (stage 3A) without albuminuria, suggesting albuminuria as a key indicator of risk in early CKD.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The presence of albuminuria in early CKD should prompt enhanced cardiovascular risk assessment, as it identifies patients with a prognosis similar to those with more advanced renal impairment.
Routine albuminuria testing in early CKD could improve cardiovascular risk stratification, supporting proactive management strategies to mitigate the risk of adverse cardiovascular outcomes.
Introduction
Chronic kidney disease (CKD), defined by an estimated glomerular filtration rate (eGFR) of <60 mL/min per 1.73 m2 body surface area, is an established risk factor for cardiovascular disease (CVD), even in the absence of albuminuria.1 2 However, there is inconsistent evidence about the relationship between CVD and the early stages of CKD, defined as stage 1 (eGFR >90 mL/min per 1.73 m2 with albuminuria, haematuria or abnormal renal morphology) and stage 2 (eGFR 60–89 mL/min per 1.73 m2 with and without albuminuria) despite these being more prevalent than the later stages of CKD.3–7 Albuminuria, particularly in the macroalbuminuric range, has been consistently recognised as a risk factor for future cardiovascular events and mortality, independent of traditional vascular risk factors such as hypertension and diabetes.8 The mechanisms underlying the association between albuminuria and CVD are largely unknown, but it is possibly a marker of endothelial dysfunction and microvascular damage, inflammation or subclinical atherosclerotic processes.9–11
The term ‘cardiorenal syndrome’ was proposed to define a clinical trajectory with kidney and cardiac impairment. Left ventricular hypertrophy (LVH) and associated myocardial fibrosis is a key feature and an established determinant for sudden cardiac death in patients with CKD.12 Several cohort studies that included patients with advanced CKD have sought to characterise the association between CKD and CVD. A meta-analysis investigating the impact of albuminuria on all-cause mortality found that a lower eGFR and a higher level of albuminuria were independent risk factors for all-cause mortality in high-risk patient groups.13 However, there are limited data on such associations in community-based populations and the contribution of measured albuminuria in the early stages of CKD.
Despite being a robust predictor of both CKD and CVD outcomes, albuminuria is an under-recognised component of the definition, staging and prognostication of CKD compared with eGFR. To bridge the gap in the current knowledge base, we sought to investigate whether the presence or absence of albuminuria in the early stages of CKD could be used to predict future cardiovascular events among community‐based participants of the UK Biobank (UKB) cohort. We also investigated the relationship between albuminuria and left ventricular mass (LVM) in a subset of participants who subsequently received cardiovascular magnetic resonance (CMR) imaging. We hypothesised that stage 1 and stage 2 CKD with albuminuria are associated with a higher risk of developing clinical CVD compared with participants with a normal eGFR (defined as ≥90 mL/min per 1.73 m2 in the absence of albuminuria).
Methods
UKB is a prospectively recruited population-based cohort of over 500 000 individuals enrolled between 2006 and 2010.14 A wealth of data on demographic and lifestyle factors, medical history and a range of physical measurements and biological samples were collected from participants. From 2015, a subset of the original UKB study volunteers were recalled for a whole-body imaging study including dedicated CMR examination.15 This study is covered by the overall ethical approval for UKB studies from the NHS National Research Ethics Service on 17 June 2011 (Ref 11/NW/0382) which was extended on 18 June 2021 (Ref 21/NW/0157).
We calculated eGFR using serum creatinine and the CKD-EPI 2021 equation and albuminuria was ascertained by the urinary albumin-creatinine ratio (ACR), defined as ACR ≥3 mg/mmol.16 In this study, the primary endpoint was MACE, defined as either hospitalisation or death due to fatal/non-fatal myocardial infarction, stroke or ventricular arrythmia. Cases were identified using relevant International Classification of Disease, 9th or 10th Revision (ICD-9, ICD-10), or Office of Population Censuses and Surveys V.4 (OPCS 4) Classification of Interventions and Procedures codes in the health-related records or death register (online supplemental table 1). We also performed additional analyses, testing for associations with heart failure (HF) and all-cause mortality separately. The follow-up period was determined by the first appearance of a relevant ICD-9, ICD-10 or OPSC4 code in either health record or death register data since the initial visit. Participants with prevalent events at the time of UKB enrolment were excluded from the survival analyses. Participants who did not experience an event were censored at death (last data collection date: 30 November 2022) or the end of the follow-up period (31 October 2022). LVM was calculated from CMR studies using an automated algorithm described elsewhere.17 18
Supplemental material
Statistical analyses
Participant characteristics at baseline are presented as mean±SD for continuous variables or counts (proportion) for categorical variables, stratified by CKD stages. The trends across CKD groups were tested by Cuzick’s extension of the Wilcoxon rank-sum test for continuous variables and the χ2 test for categorical variables. The distribution of continuous data was assessed by visual inspection of the histograms. For all analyses, a two-tailed p value <0.05 was deemed statistically significant.
We used Kaplan-Meier survival curves and adjusted Cox proportional hazards regression to examine the relationships between CKD stages and MACE, HF, combined MACE and HF, and all-cause mortality, controlling for the confounding effects of age, sex, ethnicity and cardiovascular risk factors including body mass index, hypertension, dyslipidaemia, diabetes mellitus and smoking. The assumption of proportional hazards was assessed by visual inspection of the Schoenfeld residuals.
In secondary analyses, we first assessed for an interaction between the relationship of CKD stages with cardiovascular outcomes and the presence of albuminuria. Subsequently, in a subgroup restricted to participants with stage 2 CKD, we examined the effect of varying severity of albuminuria (A1=ACR<3 mg/mmol, A2=ACR of 3–30 mg/mmol and A3=ACR>30 mg/mmol) on cardiovascular outcomes using Cox models adjusted for the same covariables as in the primary analyses. In a separate analysis, we accounted for the potential competing risk of death on the relationship between CKD stages and cardiovascular outcomes using a subdistribution hazards model based on the approach of Fine and Gray.19
In addition, to explore potential mechanisms linking CKD stages with cardiovascular outcomes, we evaluated the differences in LVM indexed to body surface area (LVMi) between early CKD stages, compared with normal renal function, using a weighted linear regression model controlled for the same covariates as the Cox models plus prevalent coronary artery disease. As the imaging subcohort had a much smaller sample size (LVMi N=40 966), we grouped CKD stages into four categories: stage 1, stage 2 without albuminuria, stage 2 with albuminuria, stage 3 and higher (stage 3+). All statistical analyses were performed using R V.4.1.1 (https://www.R-project.org/).
Results
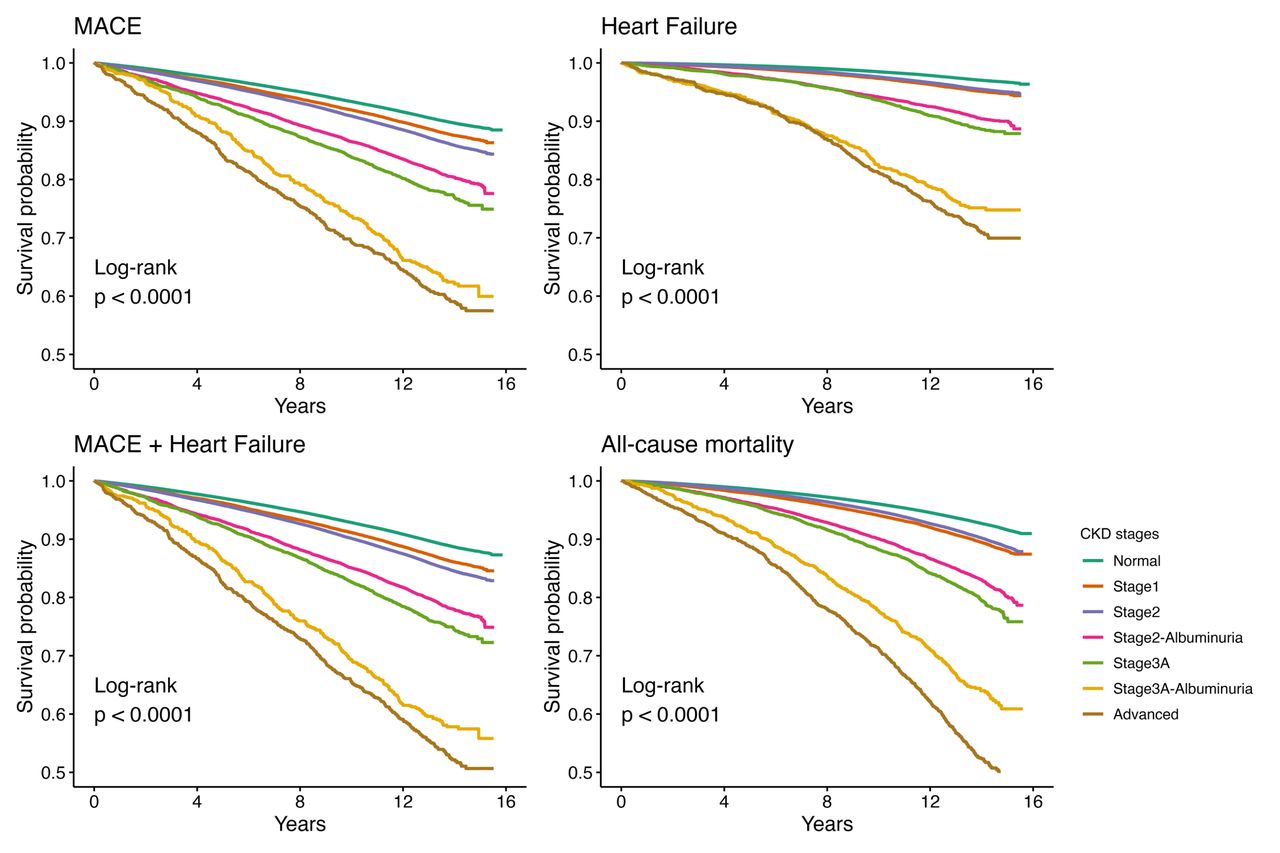
Among the participants (mean age±SD, 56.5±8.1 years), 283 121 (62.0%) had normal kidney function, 33 582 (7.4%) had stage 1 CKD, 121 358 (26.6%) had stage 2 CKD without albuminuria, 10 788 (2.4%) had stage 2 CKD with albuminuria, 4654 (1.0%) had stage 3A CKD (eGFR 59–45 mL/min per 1.73 m2) without albuminuria, 1034 (0.2%) had stage 3A with albuminuria and 1478 (0.3%) had more advanced CKD, defined as stages 3B and above. As expected, the prevalences of hypertension, diabetes mellitus and hyperlipidaemia increased with the severity of CKD; similar trends were seen in most of the other relevant parameters studied (table 1). Over a median follow-up period of 13.4 years, the number of incident MACE, HF and all-cause mortality events were 55 111 (16.6%), 18 237 (4.5%) and 44 196 (9.7%), respectively. Figure 1 shows cumulative event-free survival probability, stratified by CKD stages. There was a statistically significant difference among the CKD groups, using the log-rank test, for all outcomes studied.

Kaplan-Meier survival curves stratified by chronic kidney disease (CKD) stage. MACE, major adverse cardiovascular event.
Participant baseline characteristics stratified by kidney function
Inspection of the Schoenfeld residuals confirmed that the assumption of proportional hazards was satisfied for all outcomes studied. Using Cox regression with normal kidney function as the reference group, there was a progressive increase in the HR for MACE, HF and combined MACE and HF across the stages of CKD, except for stage 2 CKD without albuminuria (table 2 and figure 2). Stage 3A CKD with and without albuminuria and advanced kidney disease showed, as expected, significantly increased hazards for all endpoints, in line with data already published.13 Furthermore, the magnitude of association between stage 2 CKD with albuminuria and MACE (HR 1.32, 95% CI 1.25 to 1.38) was comparable to stage 3A CKD without albuminuria (HR 1.29, 95% CI 1.21 to 1.38).

{kind=link}
{kind=link}
Associations of chronic kidney disease (CKD) stages and clinical outcomes. The forest plots show HRs with 95% CIs from Cox proportional hazards regression models. The diseases listed are set as the model outcome (response variable) and CKD stages as the exposure of interest, with normal kidney function as the reference group. The model was adjusted for age, sex, ethnicity, body mass index, hypertension, hyperlipidaemia, diabetes mellitus and smoking status. HF, heart failure; MACE, major adverse cardiovascular event.
Associations between CKD stages and adverse clinical outcomes
In subdistribution hazards models accounting for the competing risk of death, the HRs for the relationships between CKD stage and HF were attenuated but remained highly statistically significant (online supplemental table 2). Early CKD stages (stage 1, stage 2 with and without albuminuria, and stage 3 without albuminuria) remained significantly associated with MACE and combined MACE and HF.
In secondary analyses, interaction terms between CKD stage and albuminuria were highly statistically significant across all cardiovascular outcomes studied. In a subgroup restricted to participants with stage 2 CKD, the severity of albuminuria had a graded relationship with adverse outcomes (online supplemental figure 1).
Supplemental material
Compared with the group with normal renal function, stage 1 CKD (which by definition has albuminuria) was associated with higher LVMi and stage 2 CKD without albuminuria was associated with lower LVMi, although the magnitude of differences was small (<1 g/m2). There was no statistically significant difference in LVM in participants with higher CKD stages compared with those with normal renal function (online supplemental figure 2), although it should be noted that very few individuals in our CMR subcohort had advanced CKD, substantially reducing the statistical power in these subgroups.
Supplemental material
Discussion
In the large community population of UKB, we showed that in the early stages of CKD, the presence of albuminuria was associated with all-cause mortality, HF and MACE, independent of other traditional cardiovascular risk factors. Importantly, this study has shown that individuals with early CKD (below stage 3) without albuminuria had a comparable prognosis to normal renal function. Furthermore, in those with stage 2 CKD, the presence of albuminuria had a graded relationship with adverse outcomes, and cardiovascular event rates comparable to those with stage 3A CKD. These excess cardiovascular event rates were seen in the absence of a clinically meaningful increase in LVM in the early stages of CKD when compared with normal renal function.
Our findings are consistent with and expand on previous studies. A meta-analysis in 2010, which included more than 1 million community participants, showed that eGFR and albuminuria were associated with all-cause mortality and cardiovascular mortality, independently of each other and traditional cardiovascular risk factors.2 However, in contrast to our study, eGFR in the meta-analysis was estimated using the Modification of Diet in Renal Disease study (MDRD) equation, which has now been superseded with the CPK-EPI equation.20 The CKD-EPI equation is more accurate than the MDRD equation, particularly in cases where the GFR is high.16 Moreover, most individuals included in this meta-analysis provided dipstick urinalysis measurements which would have missed the presence of microalbuminuria (ACR 3–30 mg/mmol). However, in our study we defined albuminuria as >3 mg/mmol, therefore including participants with microalbuminuria in our analysis and found that even a low level of albuminuria was associated with future cardiovascular events. In this meta-analysis,20 there was an increase in cardiovascular endpoints between eGFR of 60 and 75 mL/min independent of proteinuria. It is possible that unlike this study where microalbuminuria was used as a marker kidney dysfunction in stage 2 CKD, the conclusion of that meta-analysis would have been similar to this study, had they used microalbuminuria as their parameter of measuring kidney dysfunction.
Despite being a robust predictor of CVD outcomes, albuminuria is an under-recognised component of the definition, staging and prognostication of CKD compared with eGFR in routine clinical practice. In a recent cohort study, the ACR screening rate was 35.1% and 4.1% in patients with diabetes and hypertension, respectively.21 As diabetes and hypertension are the two most common causes of CKD, one would have expected a far higher screening rate, particularly considering our observations. Even in the setting of a randomised controlled trial, the participation rate for albuminuria measurement was only 59.4% and 44.3% using accessible measurement tools such as postal urine collection devices and smartphone apps, respectively.22 We believe that our study will act as a powerful impetus for change towards clinical inertia about the current use of urinary albumin estimation in the risk stratification of the early stages of CKD.
Our study may also provide an explanation for a recent observational study published in 2023 from the Linked Healthcare Administrative dataset from Ontario, Canada, which included over 8 million adults.12 Hussain and colleagues studied age-specific (18–39, 40–49 and 50–65 years) associations of modest reductions of eGFR with composite adverse outcomes (all-cause mortality, any cardiovascular event and kidney failure). After a median follow-up period of 9.7 years, adverse outcomes were consistently higher for ages 18–39 compared with older groups across all eGFR and albumin to creatinine ratio categories. Our study offers novel insights proposing that the excess risk seen with a modest reduction in eGFR within the range of stage 2 CKD in younger individuals is possibly due to concomitant albuminuria.
Cardiac imaging biomarkers of left ventricular myocardial structure and function have better defined the phenotype of renal cardiomyopathy. This study allowed us to investigate cardiac morphometric changes in the early stages of CKD after approximately 7 years of follow-up. We detected small differences in LVM between the early stages of CKD that reflect the expected pathological process in the early stages of the disease. We found that participants with stage 1 CKD had a higher LVM as compared with participants with normal renal function. In individuals with CKD, LVH often develops early in the disease process and is independently associated with increased cardiovascular mortality. Further work needs to be undertaken in patients in the early stages of CKD to ascertain whether albuminuria, higher LVM and or abnormal myocardial strain patterns are independent factors that increase MACE or whether they are both part of the same underlying pathological process and therefore have a synergistic effect.
Study limitations
The strengths of our study include the large sample size with comprehensive and detailed demographic details and rigorous characterisation of eGFR by the latest CKD-EPI equation and ACR testing, which were all analysed in a single, central laboratory. However, we acknowledge certain limitations such as the potential misclassification of participants from a single eGFR and ACR level, the lack of detailed medication data at baseline and through follow-up and the under-representation of ethnic minorities.
Two consecutive eGFR and ACR measurements 90 days apart are required to properly classify CKD. Classifying CKD based on a single eGFR or ACR measurement has notable limitations. A single eGFR measurement may reflect an acute kidney injury or another transient condition rather than a chronic state. eGFR is influenced by a multitude of factors including hydration status, recent protein intake, muscle mass, age, sex, ethnicity and medications. In addition, increases in ACR measurements may be transient due to factors such as exercise, fever, infections or recent high dietary protein intake. This may lead to overdiagnosis in individuals with transiently reduced eGFR or elevated ACR without underlying CKD. Conversely, this may also lead to underdiagnosis in cases where the eGFR and ACR levels fluctuate near diagnostic thresholds. However, in large datasets such as this as well as in mass screening programmes, single measurements have been used effectively.12 20
We were unable to access participants’ detailed medication record at baseline as well as subsequent changes in dosages and changes in medications. In the absence of these data, we were unable to robustly characterise post-enrolment changes in their CKD stage status. Certain medications such as renin angiotensin aldosterone blockers and sodium-glucose transport protein 2 inhibitors may have impacted cardiovascular endpoints as well as the progression of CKD and modulation of proteinuria. Due to the nature of a nationalised health service in the UK, we would expect that the medications used by participants in the current study cohort would broadly adhere to national recommended guidelines. This may minimise the impact of the lack of medication data on the overall findings of this study. Despite this, we recommend that in the future, pragmatic randomised controlled trials could be used to address this weakness.
Another important limitation is that the UKB cohort is predominantly white European, despite approximately 82% of the British population identifying as white, resulting in an under-representation of ethnic minorities in our cohort, limiting its generalisability. Further work is therefore required to understand whether the relationships observed in this study hold in other ethnicities. We note that there are disparities in the prevalence and management of CKD between ethnic groups and recommend that future work takes this variability into consideration at the recruitment stage to ensure better representation of ethnic minorities.23 Nonetheless, proteinuria has the same prognostic significance in patients with essential hypertension, a key risk factor for CKD, regardless of their ethnicity.24 In this context, our finding of microalbumuria as a risk factor for MACE is relevant for all ethnicities.
Conclusions
The presence of albuminuria is associated with MACE, HF and all-cause mortality in the early stages of CKD. To better risk-stratify patients for prognostication and early treatment, stage 1 and 2 CKD should be considered a significant cardiovascular risk factor only in the presence of albuminuria. Effective therapies to attenuate the complications of elevated albuminuria is expanding to include sodium-glucose transport protein 2 inhibitors, glucagon-like peptide 1 receptor agonists and endothelin receptor antagonists, in addition to renin angiotensin aldosterone blockers. In patients undergoing kidney function assessment, albuminuria testing should be an essential part of the diagnostic workup to enable better prognostication of patients with early stages of CKD.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The data underlying this article were provided by the UK Biobank under access application 2964. UK Biobank will make the data available to bona fide researchers for all types of health-related research that is in the public interest, without preferential or exclusive access for any persons. All researchers will be subject to the same application process and approval criteria as specified by UK Biobank. For more details on the access procedure, see the UK Biobank website (http://www.ukbiobank.ac.uk/register-apply/).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the NHS National Research Ethics Service on 17 June 2011 (Ref 11/NW/0382) which was extended on 18 June 2021 (Ref 21/NW/0157). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This study was conducted using the UK Biobank resource under access application 2964. We would like to thank all the participants, staff involved with planning, collection and analysis, including core lab analysis of the CMR imaging data.
References
Footnotes
KY and HN are joint first authors.
NA and MMY are joint senior authors.
X @hafiz_naderi
Contributors KY and HN contributed equally to the study and are join first authors. They co-wrote the first draft of the manuscript. HN, RJT and NA performed the statistical analyses and interpreted the data. RJT, DA, MTJ, PBM and SEP critically reviewed and revised the manuscript. NA and MMY contributed equally to the study and are joint corresponding authors. They conceptualised the project, supervised the research team, critically reviewed and revised the manuscript and attest that all authors listed meet the ICMJE authorship criteria, and that no others meeting the criteria have been omitted. They are the study guarantors.
Funding HN acknowledges the National Institute for Health and Care Research (NIHR) Integrated Academic Training Programme, which supports his Academic Clinical Lectureship post (CL-2024-19-002). SEP acknowledges the British Heart Foundation for funding the manual analysis to create a cardiovascular magnetic resonance imaging reference standard for the UK Biobank imaging resource in 5000 CMR scans (www.bhf.org.uk;PG/14/89/31194). SEP and PBM acknowledge support from the National Institute for Health and Care Research (NIHR) Biomedical Research Centre at Barts (NIHR202330). SEP has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No 825903 (euCanSHare project). N.A. acknowledges support from Medical Research Council for his Clinician Scientist Fellowship (MR/X020924/1). MMY acknowledges funding from the Diabetic Kidney Disease Centre (Ref: 577/2349).
Competing interests SEP provides consultancy to and owns stock of Cardiovascular Imaging Inc, Calgary, Alberta, Canada.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.